
• Joint pain/wear and tear
Also called cervical spondylosis, a type of arthritis in you neck. This occurs naturally with age, and does not always cause symptoms. However, some cases it can cause pain, stiffness and occasionally pins and needles or numbness in area of the arms or hands. Physiotherapy can help in most cases of cervical spondylosis.
• Slipped disc/pinched nerve
A pinched nerve, also known as cervical radiculopathy is commonly caused by a bulging or slipped disc and can result in pain in the neck, shoulder area or down the arm. Physiotherapy can be effective in treating this condition, although some cases may require surgery.
• Wry neck
Also known as acute torticollis. It is thought to be caused by acute local joint and muscle irritation which results in pain and spasm in the neck muscles. Although the exact cause of acute torticollis is unknown, it may be down to poor posture whilst sitting/sleeping or carrying heavy or uneven loads. Symptoms can usually resolve on their own within 24-48 hours, but it is advisable to try gentle movement within comfort, taking painkillers, application of heat and/or cold and focusing on maintaining good sleeping (usually one low, firm pillow is advised) and sitting posture. Physiotherapy can help if your symptoms fail to settle within a day or two.
• Whiplash
Neck injury caused by the sudden movement of the head on the neck which happens after sudden impact, for example a road traffic accident. The movement can be forwards, backwards or sideways. The symptoms caused by whiplash can be quite varied, but can certainly include pain, and tenderness in the muscles of the neck, neck stiffness and headaches.
Back pain is something which affects more than 80% of people sometime in their life. It is the leading global cause of disability - it occurs in similar proportions across cultures - and is the leading reasons for GP visits in the UK. There are many specific causes for low back pain, for example:
• spondylosis - joint wear and tear resulting in pain and stiffness in the low back
• slipped or bulging disc - can result in local low back pain, and could cause pinching of a nerve which can result in sciatica (pain referral and/or pins and needles or numbness in the buttock or parts of the leg)
• Ankylosing spondylitis - a long-term inflammatory condition of the spine and sacroiliac joints
• “non-specific low back pain”
Most cases of low back pain can resolve on their own, but most do improve or resolve more quickly with a course of physiotherapy.
Pain which is felt in the area of the back from the bottom of the neck to the top of the lower back, and can be caused by a number of issues ranging from muscle spasm or strain to vertebral fractures or collapse due to osteoporosis. In most cases the pain is self-limiting (i.e. resolves on its own), but more prolonged or severe periods of pain may require diagnostic tests and pain management strategies.
There are many types and categories of headaches, some of which can be helped by physio, others of which can’t. Examples of different types of headaches are as follows:
• Migraine
• Cluster headaches
• Head trauma
• Substance withdrawal
• Sinusitis
• Cervicogenic headaches
• Tension-type headaches
Physiotherapy can be effective in treating last two on the list above, i.e. cervicogenic and tension-type headaches. Assessment and deeper questioning helps with diagnosing the type of headache and figuring out the most effective treatment or management strategy.
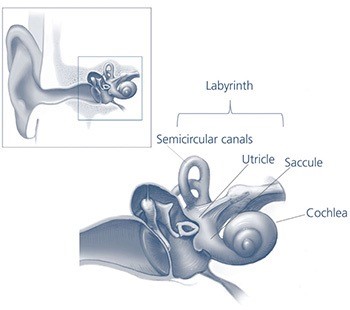
The Human Ear
Picture Credit: NIH Medical Arts
Benign Paroxysmal Positional Vertigo is a form of position-related dizziness - a spinning sensation which occurs when the position of the head is changed. Within our inner ear (also referred to as the labyrinth) lie otoconia or otoliths, also known as “ear rocks, which are small crystals of calcium carbonate. In patients with BPPV the otoconia are dislodged from their normal position in the saccule and migrate over time to the semicircular canals. The veritgo experienced with BPPV results from the movement of the otoconia in the inner ear in response to changes in head position in reaction to gravitational forces.
The vertigo associated with BPPV is sudden in onset, but is short-lived and most commonly occur with looking up or rolling over in bed. The symptoms can be made worse with changes in barometric pressure, stress and increased tiredness. Diagnosis is confirmed by the overall picture and presentation of symptoms as well as by performing a test called the Dix-Hallpike test and can be quite effectively treated by performing a set of movements and positions of the head in a particular sequence, called the Epley manoeuvre, or the Semont manoeuvre. Both manoeuvres are equally effective and aim to reposition the otoconia to an area within the inner ear where they will no longer cause symptoms of vertigo. Both manoeuvres can be taught to the patient, but the Epley manoeuvre is slightly more effective than the Semont manoeuvre when performed at home. Some patients require just one treatment, others may require multiple treatments, and symptoms can recur (which is why it is useful for patients to be taught the manoeuvre to enable self-treatment).
TMD is associated with a problem in the chewing muscles of the jaw, and can result ing pain coming from the jaw joint. Symptoms can be earache which doesn’t settle with repeated courses of antibiotics and persistent toothache (where the dentist is unable to identify a problem with the teeth). Both can be eased with a course of physiotherapy, which should include techniques to manage stress.
Impingement
Pain felt at the front of the shoulder and within the shoulder joint when lifting the arm overhead can frequently come from tendons within the shoulder being trapped between some of the moving parts of the shoulder joint. This can also be accompanied by weakness, and can be helped by resting the shoulder, avoiding aggravating activities and by taking painkillers (this should always be discussed with your pharmacist of GP first). Physiotherapy can be effective in helping to ease symptoms and restore strength in the shoulder.
Frozen Shoulder
Progressive
stiffness and pain in the shoulder, which gradually worsens over the course of months. This condition tends to be what is
called “self-limiting”, where the symptoms will gradually get better on their own. This can
unfortunately take up to 18-24 months. Generally
speaking, physiotherapy can only help to ease a patient’s pain caused by the processes happening in the
shoulder, unfortunately it can not speed up recovery. Corticosteroid
injections may be offered to help ease symptoms, and in cases where symptoms have not improved after
six months, the patient may be offered surgery.
Dislocation
Shoulder dislocation can either be due to trauma or it can happen if a person has joint hypermobility. Most often, a shoulder is dislocated during contact sports and presents with high pain levels, reduced mobility, and the shape will be different to the other shoulder - it will look more square as opposed to rounded, If you think you have dislocated your shoulder, don’t try to pop it back in place as you could damage nerves and blood vessels, rather you must go to your nearest A&E department.
A dislocated shoulder is treated by reduction under sedation (usually after the diagnosis is confirmed by X-Ray). After the shoulder has been relocated, you will need to immobilise it for a period in a sling, following which exercises to restore mobility and strength will be required.
Tennis elbow
Also known as lateral epicondylitis and presents as pain on the outside of the elbow. You may experience pain particularly with gripping activities, like pouring water from a kettle, chopping vegetables or opening jars. It usually results from overuse and is caused by inflammation or breakdown of the tissue at the tendon attachment at the side of the elbow. This condition is self-limiting, but can be very painful. Whilst waiting for recovery, physiotherapy can be useful in maintaining movement and managing pain. Additionally, a brace or strap applied around the forearm near the elbow crease can help.
Golfer’s elbow
Also known as medial epicondylitis, and as with tennis elbow (above), pain is caused by degeneration of the tendon attachment at the inside of the elbow. Treatment is similar to that of tennis elbow.
Carpal tunnel syndrome
A syndrome which causes tingling and/or numbness in the hand and fingers. These symptoms usually develop gradually and are usually worse at night. Most commonly the index and middle fingers are affected and the symptoms mentioned above could be accompanied by weakness in the thumb. Carpal tunnel syndrome occurs more commonly in those with a family history, pregnancy, diabetes, and rheumatoid arthritis. Symptoms can sometimes settle on their own, or by reducing causative factors, and non-surgical approaches like steroid injections or splints can help. Surgery may be required in cases which don’t settle, or if there is evidence of weakness or risk of permanent nerve damage.
DeQuervain’s Tenosynovitis
Pain located on the thumb-side of the wrist which is caused by activities involving turning your wrist, making a fist, or gripping things. Pain resulting from De Quervain’s tenosynovitis is caused by inflammation of two of the tendons which move the thumb. The exact cause of the inflammatory response is unknown, but is usually due to an activity relying on repetitive hand or wrist movement.
Sacroiliac Joint (SIJ)
The
sacroiliac joints are located on either side of the sacrum, which is at the
bottom of the spine between the last
lumbar vertebra and the coccyx. The SIJ’s have a shock absorbing role in movement of the body, but
usually only move a few millimetres. Pain arising from the sacroiliac joints can generally be
due to one (or both) of the joints not moving enough, or moving too much. The pain can be local to
the area, or can refer to the buttock/s or down the leg/s.
Pelvic Girdle Pain (PGP)
PGP is the term used for pain occurring in the front or back of the pelvis. This condition was previously referred to as SPD (symphysis pubis dysfunction), but was changed a few years ago as it tends to infer that the pain is caused solely by the joint at the front of the pelvic area (the pubic symphysis). What has been found, in fact, is that the pain can arise from any number of structures around the pelvic girdle. PGP can commonly occur during or after pregnancy. Previously it was assumed that the pain was caused by the relaxing effects of hormones released during birth and breastfeeding, but this has been found to be an erroneous assumption, and is more likely to be due to movement dysfunction at one (or possibly both) of the sacroiliac joints or t the pubic symphysis. This condition, although incredibly painful and debilitating, can be very effectively treated by an appropriately trained physiotherapist, where they will focus on restoring more normal movement patterns and prescribe appropriate strengthening exercises. In addition, the physiotherapist will teach you ways of managing your symptoms yourself.
Impingement
Known as femoroacetabular impingement (FAI), this condition refers to pain caused deep within the hip and is caused by one element of the hip joint pinching against the other. This usually results from the hip being an abnormal shape, it can affect up to 30% of the general population and up to 90% of certain sporting individuals. Often the individual is unaware of the problem in the early stages, so goes undiagnosed for years, but FAI increases the risk of developing hip osteoarthritis in later years. Diagnosis is made by taking a history, doing a physical examination and performing X-Rays and MRI scans of the hip.
There are two types of FAI: cam or pincer (or you can get a mixed presentation):
Cam impingement is caused by the head or neck of the femur (ball part of the ball and socket-type hip joint) being misshapen and jamming onto the socket part of the hip joint (the acetabulum), thus causing pain during certain hip movements and positions
Pincer impingement is caused by the socket of the hip (the acetabulum) is too deep, which results in contact being made by the neck of the femur, in time causing pain.
Treatment of FAI may result in surgery if conservative methods of treatment, like physiotherapy, fail.
Labral tear
The labrum of the hip is a ring of cartilage and connective tissue which runs around the rim of the hip socket (acetabulum), and is involved in cushioning the hip joint and contributing to hip joint stability. A tear can occur in the cartilage, sometimes due to a fall or car accident, and are more common in women. It can also develop from repetitive sports, and people with abnormal hip structure can be more likely to develop a labral tear, although the majority of cases have no known cause. Symptoms from a labral tear can include pain in the groin, or catching or clicking in the hip socket. Labral tears left untreated have been linked with the development of hip osteoarthritis.
Trochanteric bursitis
Inflammation of the trochanteric bursa is called trochanteric bursitis. A bursa is a fluid-filled double-layer membrane, and exits to reduce friction and act as a shock absorber between two structures in the body. The trochanteric bursa is located between the side of the hip (the greater trochanter of the femur) and the insertion of some of the gluteal muscles’ tendon onto the bone. Sometimes the bursa inner membranes of the bursa itself can become inflamed and results in pain at the side of the hip. The cause of the bursitis can be due to overuse or overloading, or sometimes there is no definable cause. Typical symptoms are pain at the side of the hip/upper thigh with walking, or lying on that side. Recent research has found, however, that pain in this area is more often associated with tissue injury to the gluteal tendons at their attachment onto the side of the femur.
Arthritis
Osteoarthritis (OA) refers to the degeneration and eventual breakdown of the cartilage lining of a joint. each joint surface is lined by a layer of cartilage and over time, normal wear and tear can sometimes accelerate to the point of cracks appearing in the cartilage. This results in varying degrees of roughening and eventual exposure of the underlying bone. This then results in abnormal loading patterns within the joint, and roughening of the joint surfaces. The most common symptoms are joint stiffness and pain. Initially, these symptoms may only occur after exercise, but may become constant as the joint disease progresses. Rest tends to ease the pain, but the patient often complains of stiffness on movement after rest. Symptoms can be helped by maintaining low-grade regular exercise (mainly to prevent excessive loss of strength), and risk is greater in those who are overweight. Treatment includes exercise, support groups and pain medication. If the pain reaches a point where it is significantly affecting quality of life, joint replacement surgery may be recommended. Although outcomes of joint replacement surgery are for most people good, an artificial joint only lasts a limited length of time.
Osteoarthritis of the hip is very common and can affect one or both of the hips. The incidence in men and women with hip OA is pretty equal, and usually starts from the late 40s onwards. Symptoms include pain deep within the front of your hip/groin, in your buttock, or at the side or front of your upper thigh.
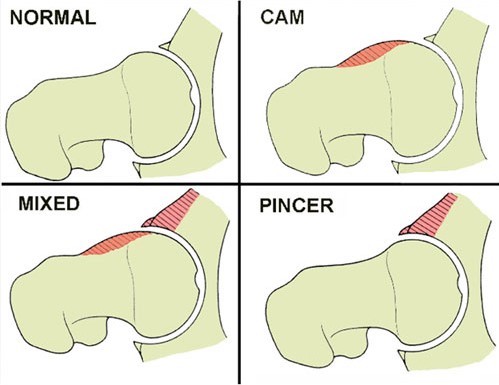
Image
credit www.jointpain.md
Cruciate ligament tears
There are two cruciate ligaments in the knee - the anterior cruciate (ACL), and the posterior cruciate (PCL). The ACL is injured more often than the PCL, and the most common injury to this structure is a complete rupture of the ligament, usually following a pivoting movement, landing from a jump, or during sudden deceleration. ACL deficient patients tend to fall into one or two categories; those who are able to return to activity and those who have persistent symptoms and instability. Those who do manage to return to activity tend to need a course of rehabilitation to strengthen the muscles around the knee to compensate for the deficient ligament, which could take several months. Those who have on-going symptoms may require reconstructive surgery. The general timeframe for people following ACL reconstruction is 4-6 months to return to running, 6-9 months to return to activities that involve changing direction and 9-12 months to return to competitive sport.
Patients will often describe hearing a pop or crack followed by immediate pain when the ACL ruptures. More often than not the patient will not be able to continue with the activity, and the knee will then normally swell very rapidly with the swelling being contained in and around the knee. Often the knee is difficult to assess in the acute stage, but an X-ray may be taken and some indications of an ACL rupture may be present. For an accurate diagnosis the patient will need to be assessed by their GP, a physiotherapist or an orthopaedic surgeon and may require a MRI scan.
If the patient manage to return to sport following the injury they will often describe a feeling of instability (giving way), usually during changes of direction or pivoting and sporting activities. There is a possibility of other structures being injured alongside the ACL, most commonly the meniscus, which may add symptoms including catching, locking, painful clicking, and recurrent swelling.
In all cases of ACL injury physiotherapy is essential. Non-surgical patients will require guided rehabilitation with a strong focus on strengthening, stability training and sport specific exercises, and patients who undergo ACL reconstruction will require on average 6-9 months of regular physiotherapy to guide them through the stages of rehabilitation, which should include advice on the protection and maximisation of the rebuilt ligament as well as guidance regarding return to sport.
If you suspect you have sustained an ACL injury it is very important you follow the PRICE principal immediately after the injury. That is you rest the knee ideally with the protection of a brace, ice it, apply gentle compression and elevate it, and go to A&E. For those not undergoing reconstructive surgery you will need to spend time focussing on strengthening your quadriceps, hamstrings and core stability muscles as well as improving your balance.
If you have sustained an ACL injury in the past and you continue to have symptoms and have not managed to return to your desired level of activity you should see your GP with the view of being referred to an orthopaedic consultant.
Meniscal tears
The meniscus is a cartilage structure within the knee. Its function is to help with shock absorption and to reduce friction. The most common way this structure is injured is by twisting the knee on a planted foot. The meniscus can also become frayed and injured through general wear and tear and the degeneration process.
Following a meniscal injury the patient will often report a build-up of swelling and pain over a period of 24 hours. They will often have tenderness along the sides of the knee and can have a painful clicking when moving the knee. Sometimes the knee will also become locked, meaning you are unable to fully straighten or bend the knee. The patient may also complain of a feeling of instability in the knee during daily activities or sport.
In the acute phase following a meniscal injury physiotherapy can be helpful in providing and accurate diagnosis and in helping with pain management. Some minor meniscal injuries can be managed conservatively, that is through physio treatment and prescription of appropriate exercises. Others may need to go on to have surgery, which is usually done via arthroscopic (keyhole) surgery, and normally has a quick recovery time. Post operatively physio is very helpful in helping to regain full strength, range of movement, and return to full activities of daily life and sports. The general recovery time following meniscal surgery is between 2-3 months.
If you suspect you have injured your meniscus icing, resting and elevating the knee especially in the first 72 hours would be very beneficial. Trying to maintain you thigh muscle strength will really help to speed up your recovery. This can be achieved by lying with your leg out straight on the bed, then tensing the thigh muscle by pressing the back of the knee into the bed. Try to maintain this squeeze for 5 seconds and repeat the exercise 15 times.
It is advisable to see your GP for onward referral to a physio or to an Orthopaedic Surgeon if you suspect a meniscal injury.
Jumper’s knee
Also known as patellar tendonopathy, this condition is characterised by degeneration of the structure of the patellar tendon (running from the bottom tip of the knee cap to the shin bone) and may or may not have associated inflammation. This condition most commonly develops from a sudden change in activity, an increase or decrease in training or in the presence of a biomechanical issue like poor foot posture, inappropriate footwear or reduced core stability. Patellar tendonopathy can result in long term absence from activity and sport and, if left untreated, can worsen requiring, in some cases, surgical intervention. Apart from sporting overuse, this condition is also associated with ageing. As we get older, our ability to regenerate damaged tissue decreases and the quality of the tendon deteriorates.
Symptoms usually develop gradually and is characterised by pain at the front of the knee, just below the kneecap. The pain is worsened by activity, and the focal areas of degeneration feel tender to touch. Often the tendon feels very stiff first thing in the morning. The affected tendon may appear thickened in comparison to the unaffected side. Any exercises that load the patella such as going up and down stairs, squatting, kneeling and repetitive impact can all aggravate the tendon. Prolonged driving and sitting can also cause stiffness and pain in the knee as the tendon is placed on strain with a bent knee.
Physiotherapy treatment will often involve correcting inappropriate training practices, advice on footwear, massage, stretches, strengthening exercises to the knee, hip and core, acupuncture, taping, and electrotherapies. The therapist will check if there is a biomechanical issue affecting stresses placed through the knee. It may be appropriate to then refer you to an orthotist or podiatrist for some inserts for you shoes.
Avoid impact exercises that aggravate your symptoms and apply ice to the tendon during the early stages of your injury. Maintain quadriceps flexibility and wear appropriate footwear for your sport. You can buy patella tendon braces that help to offload the tendon, they can be worn during sport which will help to relieve your symptoms.
ITB friction syndrome
The ITB is a tough fibrous structure which runs down the outside of the leg from the hip to the knee. ITBS is a common overuse running injury, and occurs when there is excessive friction between the band and the bony outside edge of the knee. It is caused by inadequate control of the mechanics around the knee, which in turn results from poor foot posture during running, inadequate hip control or poor core stability. Symptoms usually include pain which comes on during running and is located at the outside of the knee. Traditional types of treatment focused on trying to alter the length of the ITB through stretching or foam rolling, but recent research suggests that the ITB is actually a tendinous- type structure which is overloaded through poor control of pelvic stability. As a result, it appears that a better approach to managing this problem is to focus on correcting of the source of pelvic instability - for example, gluteal muscle strengthening, the assessment for the use of orthotics (inserts for your shoes), and improvement in core stability.
Arthritis
Osteoarthritis (OA) is the most common form of arthritis. It usually develops gradually, over time. Several different joints can be affected, but osteoarthritis is most frequently seen in the hands, knees, hips, feet and spine. There is no known cause for osteoarthritis, but it is more common among women. Osteoarthritis can develop at any age, although it occurs more frequently in older people. Although it is not common to get osteoarthritis under the age of 40, around 80% of over 75 year olds have arthritis. Diagnosis rates are highest in people from the age of 40-50. Injury to a joint can also trigger osteoarthritis, even many years later. Osteoarthritis develops when part of the cartilage breaks away from the bone leaving the bone ends exposed. These may then rub against each other and the ligaments become strained and weakened. This causes a lot of pain and changes the shape of the joint causing inflammation of the synovial membrane. Common causes of osteoarthritis include: obesity, previous joint injury, joint overuse, and genetic disposition. Osteoarthritis cannot be cured, but the condition may settle down after a number of years and there is plenty you can do to relieve your symptoms. As osteoarthritis develops over time, changes will be slow and subtle in some people, whereas in others, the pain and stiffness will gradually worsen until the disease process finishes. At this point, the joints will look rather knobbly, but are usually far less painful. In some cases they become pain free. You should be able to carry out most everyday tasks. You may need an X-ray to confirm the arthritis.
Your doctor can prescribe you one (or more) of the following types of drugs: analgesics (painkillers) which relieve pain, non-steroidal anti-inflammatory drugs (NSAIDs) which reduce inflammation and, in turn, steroids, which also reduce inflammation, and can be directly injected into a joint for fast relief. Your doctor may refer you to an orthopaedic surgeon if you have severe arthritis affecting weight-bearing joints, such as the knees and hips. If you do have your joints replaced they should last for 15-20 years. But in people who are more active the artificial joint may wear out sooner. If a joint becomes loose, wears out or develops a complication, a revision operation can be performed to replace the joint.
Doing exercises to strengthen your muscles will reduce pain and stress on your joints – a physiotherapist can help with this. Common low impact exercises like swimming, walking and cycling allow you to strengthen the muscles without aggravating the symptoms, massaging painful joints and muscles can help with pain management, losing weight if you are overweight helps to reduce strain on your weight-bearing joints, and complementary therapies such as acupuncture and aromatherapy can also help with pain reduction.
Arthritis Care run a range of self-management programmes designed to teach you skills to live life to the full and to help you get the most out of your healthcare team. The courses also allow you to meet other people with your condition. The Arthritis Care Helpline is available to answer any specific questions you may have on all aspects of arthritis.
Ankle sprains
Feet
Achilles tendonopathy
Often referred to as achilles tendonitis. This condition is characterised by a degeneration of the structure of the Achilles tendon and may or may not be accompanied by inflammation. Achilles tendonopathy most commonly occurs when there is a change in activity, an increase or decrease in training or in the presence of a biomechanical issue like poor foot posture, inappropriate footwear or reduced core stability. Achilles tendonopathy can be the cause of long term absence from activity and sport and, if left untreated, can worsen requiring, in some cases, surgical intervention.
Patients suffering from Achilles tendonopathy often report intense pain located around the back of the ankle, usually along the length or at the base of the Achilles tendon which runs upwards from the heel bone into the calf. This pain is usually worse during the start of activity, settles once the patient gets moving and returns as the patient continues with the activity. Patients may notice a lump or nodule along the tendon. Some patients may get relief from anti-inflammatory medication but many will not. Flat unsupportive footwear will often make the pain worse.
Physiotherapy can quite often be effective in the treatment of achilles tendon problems, where treatment will often involve correcting inappropriate training practices, advice on footwear, massage, stretches, strengthening exercises and electrotherapy.
Often shoes with a
slight heel will be more comfortable to wear day to day. If you are training
regularly you may benefit from incorporating rest days into your training
programme, adding in some cross training. This can include weights, Pilates,
yoga, or circuit classes, and varying the terrain on which you run or walk.
Making sure you stretch after exercise can also help improve or even help to
avoid developing Achilles issues. Particular focus should be on stretching the
calf muscle. A biomechanical assessment and possibly the provision of
custom-made orthotics can help correct the problem.
Plantar fasciitis
The plantar fascia is a soft tissue structure which runs under the sole of the foot, and plantar fasciitis develops when the plantar fascia thickens over time in response to injury. This can be due to a specific injury or due to a number of smaller injuries over years. More common in women than men, plantar fasciitis develops in combination with age and increased body weight, increase in the frequency exercise or exercise intensity. In addition, it can be aggravated by being on your feet all day, or can be due to wearing poorly supportive, thin-soled shoes. Abnormal foot biomechanics can also be a causative factor.
Plantar fasciitis is characterised by pain and/or tightness felt in the middle of the heel on the underneath of the foot, or along the underneath of the arch of the foot. The pain is usually worse in the morning, with long periods of walking in poorly supportive shoes, or when walking after periods of sitting.
Diagnosis is usually pretty straight forward (due to the unique nature of symptoms), and treatment can include using a heel pad to cushion the painful heel, off the shelf orthotics, or custom-made orthotics can be particularly useful. Stretches can help to ease the tight structures of the foot and ankle, as well as the use of ice, ultrasound, painkillers and anti-inflammatories. The use of a night splint can help to keep the ankle at a specific angle to stop the plantar fascia from shortening whilst you are sleeping. If all these approaches fail, you may be offered a course of shockwave therapy or cortisone injection.
Please understand that taking calls during the day is difficult as I am usually with patients, so text or email is my preferred method of contact. Thank you.
© Elite Performance Physiotherapy 2020. All rights reserved
For an appointment email: Info@eliteperformancephysiotherapy.co.uk
Or phone: 07714 847127